EMTT therapy in Edmonton uses electromagnetic pulses to help chronic musculoskeletal pain. Discover how Unpain Clinic combines EMTT with rehab for real results.
KEY TAKEAWAYS
- EMTT (Extracorporeal Magnetotransduction Therapy) is a non-invasive treatment that delivers high-intensity electromagnetic pulses into tissue from outside the body. It is not the same as the consumer PEMF mats sold for home use.
- The current evidence base is small but consistent. The best-designed trial to date, a 2026 double-blind placebo-controlled study in 126 patients with knee osteoarthritis, rotator cuff enthesopathy, or lumbar spondyloarthrosis, showed measurable improvements in pain and quality of life over an 8-week course.
- The clinical case for EMTT is strongest as an adjunct, layered on top of structured rehabilitation and (in many cases) alongside shockwave therapy. It is not positioned as a stand-alone treatment, and it does not replace exercise.
- A typical EMTT course is 6 to 8 weekly sessions of about 20 minutes each. Most patients feel little to nothing during treatment.
- EMTT is contraindicated for people with active implanted electronic devices (pacemakers, cochlear implants, neurostimulators), during pregnancy, and for treatment over the brain or directly over malignancies. Other contraindications apply depending on the device manufacturer's guidance.
- Severe sudden pain, fever, unexplained weight loss, neurological symptoms, or a new injury warrant a physician's evaluation before any rehabilitation work.
IN THIS ARTICLE
- What EMTT is, and how it differs from PEMF
- Why some chronic musculoskeletal pain does not respond to standard care
- What the research actually shows
- How EMTT fits into a treatment plan at Unpain Clinic
- What to realistically expect from a course
- Safety and contraindications
- FAQ
INTRODUCTION
If you have a chronic musculoskeletal pain that has not budged after physiotherapy, exercise, anti-inflammatories, maybe a cortisone injection or two, the question of whether anything else can move the needle is a fair one. EMTT (Extracorporeal Magnetotransduction Therapy) is a treatment that has been getting more attention in the last few years, partly because the published evidence has grown, and partly because clinicians who work with chronic pain have started reporting results when EMTT is layered onto existing care. This article walks through what EMTT actually is, what the published trials show, and where it sensibly fits.
The honest framing throughout is that EMTT is an adjunct, not a stand-alone fix. It does not replace structured rehabilitation. It does not replace a proper assessment of what is driving the pain. What the evidence supports is that for the right patient, in the right plan, it can add measurable improvement on top of standard care.
This is general education, not individual medical advice. If your pain is severe, sudden, new, or accompanied by fever, neurological symptoms, or unexplained weight loss, see a physician before considering any rehabilitation modality.

WHAT IS EMTT, AND HOW IS IT DIFFERENT FROM PEMF?
EMTT stands for Extracorporeal Magnetotransduction Therapy. "Extracorporeal" means delivered from outside the body. "Magnetotransduction" refers to the conversion of an applied magnetic field into a biological signal inside tissue. In practice, an electromagnetic applicator is positioned over the area being treated, and the device delivers brief, repeated high-intensity electromagnetic pulses into the tissue underneath. The patient does not feel a sharp sensation. Most people feel nothing or a faint warmth.
EMTT belongs to the broader family of pulsed electromagnetic field (PEMF) therapies, but the technical parameters are different from the consumer PEMF mats and devices sold for home use. EMTT operates at much higher magnetic field intensities (typically around 80 milliTesla in the published trials) and uses specific pulse frequencies and protocols delivered through a medical-grade applicator. The consumer PEMF market and the medical EMTT literature are not interchangeable, and results from one cannot be extrapolated to the other.
The mechanism is not a single switch. The proposed biological pathway is that the electromagnetic pulses interact with cell-membrane and intracellular signalling involved in inflammation regulation and tissue repair. Preclinical work, including the 2024 study by Gerdesmeyer and colleagues in Biomedicines, has shown that EMTT exposure can accelerate human osteoblast activity and matrix mineralisation in laboratory settings, supporting a plausible biological rationale for bone-healing applications. Broader PEMF literature has shown anti-inflammatory effects through signalling pathways including adenosine receptors and NF-kB, and support for tissue-repair biology including angiogenesis and bone formation. These findings sit alongside, and help explain, the clinical trial signal in human patients.
WHY DOES SOME CHRONIC MUSCULOSKELETAL PAIN NOT RESPOND TO STANDARD CARE?
Most people with persistent musculoskeletal pain are not doing nothing. They are usually doing a lot. Physiotherapy. Exercise. Medication. Activity modification. Maybe injections. The fact that some cases still plateau is not about effort. It is about what the standard care is and is not doing.
Standard conservative care does two main things. It restores movement, strength, and control through exercise and manual therapy. It manages the pain signal short-term with medication and sometimes injections. Both are essential. Both work for most people, most of the time.
What standard care does not directly do is change the cellular and signalling environment inside the painful tissue itself. When tissue stays inflamed or irritated for weeks or months, local biological pathways can settle into a state where repair does not progress at the rate it should. Tendons do not remodel cleanly. The local pain signal stays up. Function plateaus.
This is the gap that targeted regenerative adjuncts (shockwave therapy and EMTT among them) are designed to address. They do not replace the exercise work and the strength gains that rehabilitation builds. They add a tissue-level biological stimulus that, when layered onto the rest of the plan, can shift outcomes for cases that have stalled.
At Unpain Clinic, the pattern we see most often with patients who fit this description is the same. Movement is better than when they started. Strength is improved. But pain has plateaued at a level that interferes with sleep, work, or the activities they care about. EMTT is one of the tools we use to help close that last gap, and only as part of a structured plan.

WHAT DOES THE RESEARCH ACTUALLY SHOW?
The EMTT evidence base is small relative to older modalities like physical therapy or shockwave therapy, but it is growing, and the most recent and best-designed trial is also the most informative.
The strongest current evidence comes from the 2026 double-blind placebo-controlled randomised trial by Hollander and colleagues in the Journal of Back and Musculoskeletal Rehabilitation. This trial randomised 126 patients with at least 6 weeks of pain from one of three conditions (knee osteoarthritis, rotator cuff enthesopathy, or lumbar spondyloarthrosis) to either real EMTT (delivered at 80 milliTesla, 8 Hertz, 10,000 pulses per session, once weekly for 8 weeks) or sham therapy. The primary outcomes were quality of life on the SF-12 Physical and Mental Composite Scales. The secondary outcome was pain on the visual analog scale. The EMTT group showed measurable improvements in pain and physical quality of life relative to the sham group. This trial is meaningful because it covers three different chronic musculoskeletal conditions, uses a true placebo control (with patients and assessors blinded), and is the largest published EMTT trial to date.
The earlier evidence runs in the same direction. The 2017 prospective randomised controlled trial by Krath and colleagues in the Journal of Orthopaedics examined EMTT in patients with non-specific low back pain. Both groups received the same standardised conservative care (physiotherapy plus analgesics). One group received real EMTT in addition; the other received sham EMTT. The EMTT group showed greater reductions in pain on the visual analog scale and greater improvement in disability scores on the Oswestry Disability Index at both the 6-week and 12-week assessments, with the gains holding at follow-up after the last treatment.
EMTT has also been studied in combination with shockwave therapy. The 2018 prospective randomised controlled trial by Klüter and colleagues in Electromagnetic Biology and Medicine randomised 86 patients with rotator cuff tendinopathy to shockwave therapy plus real EMTT or shockwave therapy plus sham EMTT. The combination group (real shockwave with real EMTT) achieved greater improvement in pain and shoulder function than the shockwave-only group. This is a useful design because shockwave alone is already an evidence-supported treatment for rotator cuff tendinopathy. The trial speaks to whether EMTT adds value on top of an already effective treatment, and it did.
The honest framing. The total EMTT evidence base is still small, with relatively few large multicentre trials. The trials that exist are mostly from the same European research group and are partly device-manufacturer-supported, which is a real limitation that is worth naming. That said, the trials are reasonably well designed, the results consistently favour EMTT, and the preclinical biology is plausible. The current position in the literature is that EMTT is a reasonable adjunct for chronic musculoskeletal pain that has not responded to standard care, particularly when combined with shockwave therapy or structured rehabilitation, and that more independent multicentre trials would be welcome.
"EMTT is not the headline of the treatment plan. It is the thing that, in the right case, makes the rest of the plan work better. The honest position is that it is one tool, not the whole toolbox." Uran Berisha, BSc Physiotherapy, Founder of Unpain Clinic
HOW DOES EMTT FIT INTO A TREATMENT PLAN AT UNPAIN CLINIC?
At Unpain Clinic in Edmonton, EMTT is never used as a stand-alone treatment. The conditions we use it for sit inside a structured assessment-and-plan process and run alongside other treatments selected based on what the assessment shows.
A first visit is an assessment, not a treatment session. The clinician takes a full history, examines the painful area and the surrounding kinetic chain, reviews any imaging that is available, and walks through what your specific picture suggests. If the assessment turns up something that needs a physician's involvement first (a suspected fracture, a neurological pattern, a systemic concern, a clear surgical candidate), we coordinate that referral before continuing.
For the cases where a non-surgical plan is the right starting point and EMTT may be appropriate, the toolbox we draw on is built around what the evidence supports for chronic musculoskeletal pain.
Physiotherapy with structured, progressive rehabilitation is the backbone. EMTT does not replace it. The strength, mobility, and movement-pattern work is what makes the result hold once the active treatment phase ends.
Focused shockwave therapy is the most common companion modality for EMTT in our clinic. The combination is supported by the Klüter 2018 trial in rotator cuff tendinopathy and by the broader pattern across the EMTT literature. Shockwave delivers a mechanical stimulus. EMTT delivers an electromagnetic one. The two approaches address tissue biology from complementary angles.
Radial shockwave therapy is layered in for surrounding muscle tension and trigger points that contribute to altered movement patterns.
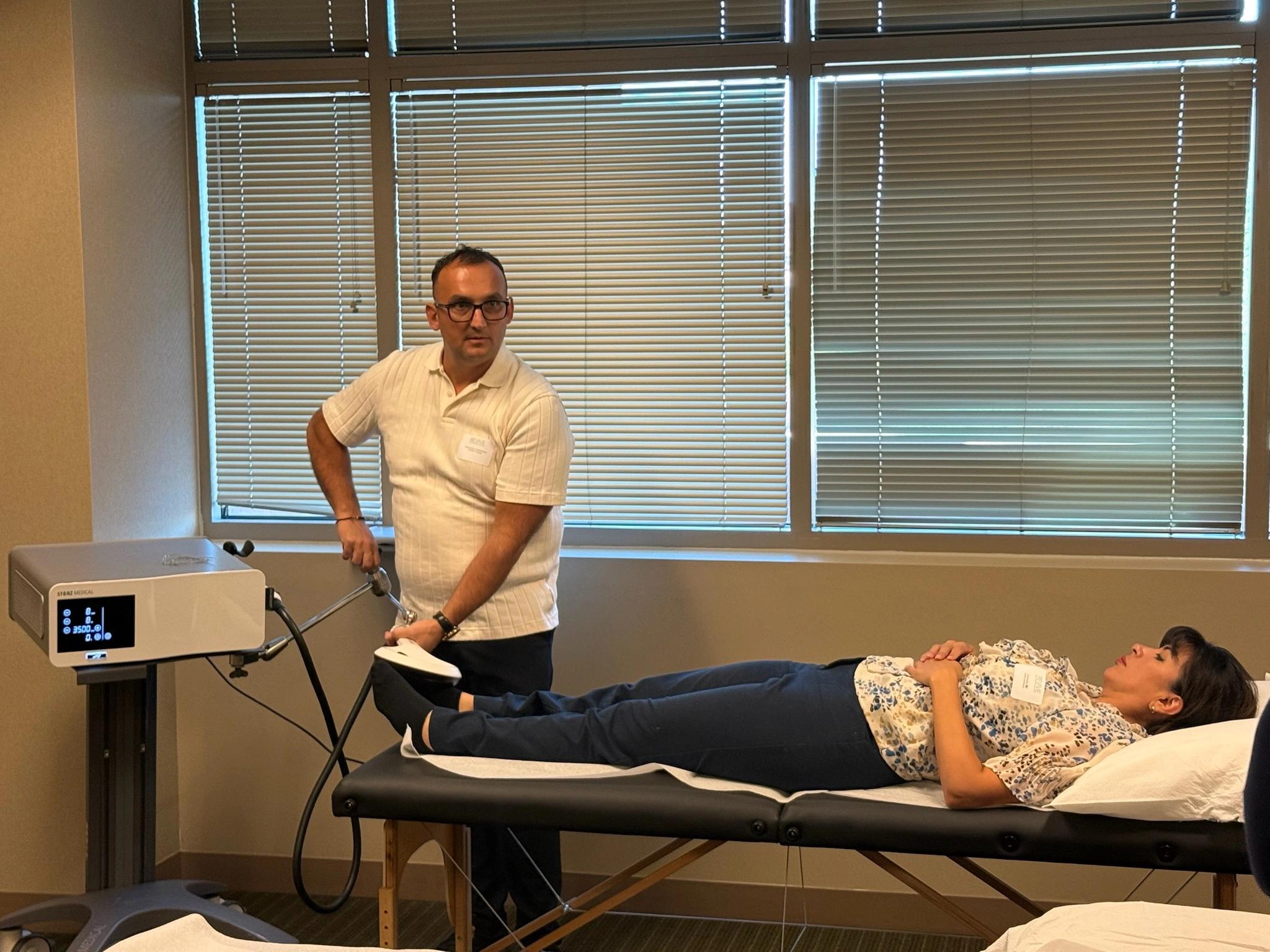
EMTT therapy is delivered through a STORZ Magnetolith applicator at protocols similar to those used in the published trials. Sessions are typically about 20 minutes, delivered once or twice weekly for 6 to 8 weeks. The exact protocol is matched to your specific condition.
NESA neuromodulation is reserved for cases where the nervous system has become hypersensitive and pain has started to outlast what the tissue findings would predict. EMTT and NESA work on different aspects of the picture and are sometimes used in combination.
For deeper looks at how shockwave and EMTT work together in specific conditions, our cluster includes shockwave therapy for back pain, shockwave therapy for stress fractures, and shockwave therapy for hip osteoarthritis.

WHAT TO REALISTICALLY EXPECT FROM A COURSE
A typical EMTT course at Unpain Clinic is 6 to 8 weekly sessions of about 20 minutes each, layered on top of the rest of the rehabilitation plan. The sensation during treatment is mild. Most patients feel a faint warmth, a light tapping sensation, or nothing at all. There is no recovery time after a session. People leave and go back to their day.
The pattern of improvement is rarely dramatic in the first session. The Krath 2017 trial measured improvements at 6 weeks and 12 weeks, with both timepoints showing meaningful gains over sham. The Hollander 2026 trial used an 8-week course and assessed quality of life and pain outcomes at and after the treatment period. The clinical reality matches these timelines. Most patients who respond start to notice the first shifts in the third or fourth week of the course, with bigger gains in the weeks after the last session as the tissue continues to respond.
Factors that influence response. How long the symptoms have been there, the specific condition (the strongest published evidence sits in lumbar spine, rotator cuff, knee osteoarthritis, and Achilles), the rest of the plan (EMTT works best layered on structured rehabilitation, not in isolation), and whether the home program is actually being done.
The boundary of what EMTT can and cannot do is worth stating clearly. It does not replace exercise. It does not regrow torn tissue. It does not change the bony anatomy of a worn joint. It does not substitute for a surgical fix when one is genuinely required. What it does, in cases that respond, is shift the local tissue biology enough that the rest of the rehabilitation work produces a better result than it would have on its own.
SAFETY AND CONTRAINDICATIONS
EMTT is non-invasive and well tolerated in the published trials, with no serious adverse events reported and only occasional transient skin redness at the treatment site. Serious adverse effects have not been reported in the trials we have cited.
That said, EMTT is not appropriate for everyone. The clear contraindications are:
- An active implanted electronic device (pacemaker, defibrillator, cochlear implant, neurostimulator, insulin pump) in the field of treatment.
- Pregnancy.
- Direct treatment over the brain or skull.
- Direct treatment over an active malignancy.
- Active infection in the treatment area.
- Severe untreated cardiac arrhythmia or other significant cardiac instability.
- An open wound or recent surgery in the treatment area without clinician clearance.
Passive metal implants (joint replacements, plates, screws) are not absolute contraindications, but they require an individualised review against the device manufacturer's guidance before treatment. Your clinician will go through this with you during the assessment.
WHEN SHOULD I SEE A PHYSICIAN INSTEAD OF (OR ALONGSIDE) EMTT?
The following are not "wait and see" situations. Contact your physician promptly, or seek emergency care if symptoms are severe.
- Sudden severe pain after a fall or specific injury.
- A clear new loss of strength or function.
- Numbness, tingling, or weakness traveling down a limb.
- Fever, hot or red joints, or feeling systemically unwell.
- Unexplained weight loss alongside the pain.
- Bladder or bowel changes with low back pain, or saddle-region numbness (possible cauda equina presentation, a medical emergency).
- A known history of cancer with new bone or joint pain.
- A pain pattern that has not responded to a fair trial of structured rehabilitation.
FREQUENTLY ASKED QUESTIONS
What is EMTT therapy and how does it work?
EMTT (Extracorporeal Magnetotransduction Therapy) is a non-invasive treatment that uses an applicator placed over the painful area to deliver brief high-intensity electromagnetic pulses into the underlying tissue. The pulses interact with cell-level signalling pathways involved in inflammation regulation and tissue repair. The treatment is generally painless and takes about 20 minutes per session.
Does EMTT hurt?
Most patients feel little to nothing during treatment. Some describe a faint warmth or a light tapping sensation. EMTT is generally well tolerated, and there is no recovery time after a session.
How many EMTT sessions will I need?
Published trials have used 6 to 8 weekly sessions, and that is the typical course at Unpain Clinic. The exact number depends on your specific condition, the rest of the plan, and how you respond to the first few sessions.
Is EMTT the same as a PEMF mat I can buy online?
No. EMTT operates at substantially higher magnetic field intensities and uses specific clinical protocols delivered through a medical-grade applicator (the STORZ Magnetolith in our case). The consumer PEMF market and the medical EMTT clinical literature are not interchangeable, and you should not expect the results from one to predict the results from the other.
Is EMTT safe?
EMTT is generally well tolerated. Published trials report no serious adverse events, with occasional transient skin redness at the treatment site as the most common minor finding. The clear contraindications are active implanted electronic devices in the field, pregnancy, direct treatment over the brain, direct treatment over an active malignancy, and active infection in the area. Other contraindications apply depending on the device manufacturer's guidance.
Can EMTT be used with a metal implant?
Passive metal implants (joint replacements, plates, screws) are not absolute contraindications, but they require individualised review against the device manufacturer's guidance before treatment. Active implanted electronic devices (pacemakers, cochlear implants, neurostimulators) in the treatment field are absolute contraindications.
Can EMTT help me avoid surgery?
There are no published head-to-head trials comparing EMTT directly to surgical interventions. EMTT is best understood as a non-invasive adjunct within conservative care, not as a proven surgery replacement. That said, if a structured conservative plan that includes EMTT resolves your pain and restores your function, surgical intervention may become unnecessary in cases where it was being considered for symptom relief rather than for a clearly structural reason. The decision belongs with you and your physician or surgeon.
How much does EMTT cost in Edmonton?
EMTT pricing varies depending on the number of sessions and what other modalities are included in your treatment plan. We provide transparent pricing at your initial assessment before you commit to anything. Contact the clinic directly for current rates and package options.
Do I need a doctor's referral to come to Unpain Clinic?
No referral is needed. Physiotherapists and chiropractors in Alberta practice as primary contact clinicians. Some insurance plans require a physician's note for reimbursement, so check your plan if you intend to claim. If the assessment turns up something that needs a physician's involvement, we coordinate that referral.
PATIENT TESTIMONIAL
"The second treatment on the knee worked wonders! The pain was gone within 1-2 hours. I played basketball last night and usually my knee is sore and puffy the next day, well it wasn't! This am I went to the gym and I was able to do a squat without the pain. I am so happy. I haven't been able to do this in so so long. It's a big deal.Can I do another treatment just to stay on top of this amazing result?? Thank you!!!"
ABOUT THE AUTHOR
Written by Uran Berisha, Founder of Unpain Clinic and Medical Shockwave Institute. Uran has a Bachelor of Science in Physiotherapy and is an International Educator in Shockwave Therapy. Last reviewed on June 11, 2026.
BOOK YOUR INITIAL ASSESSMENT
If you have a chronic musculoskeletal pain that has plateaued on standard care, and you want a clear, honest read on whether EMTT (and the rest of a structured plan) can move the picture, the next step is a proper assessment. We will look at what is actually driving the pain, walk through the options that fit your case, and tell you honestly what we expect a course of treatment to deliver. No referral needed. No long contracts. Book your initial assessment with Unpain Clinic.
REFERENCES
- Hollander K, Burgkart R, von Eisenhart-Rothe R, Vester J, Gerdesmeyer L. Extracorporeal magnetotransduction therapy (EMTT) for management of musculoskeletal disorders: A double-blind, placebo-controlled, randomised trial. Journal of Back and Musculoskeletal Rehabilitation. 2026 (Collection date May 2026). https://pmc.ncbi.nlm.nih.gov/articles/PMC13109596/
- Krath A, Klüter T, Stukenberg M, Zielhardt P, Gollwitzer H, Harrasser N, Hausdorf J, Ringeisen M, Gerdesmeyer L. Electromagnetic transduction therapy in non-specific low back pain: A prospective randomised controlled trial. Journal of Orthopaedics. 2017;14(3):410-415. https://pubmed.ncbi.nlm.nih.gov/28736490/
- Klüter T, Krath A, Stukenberg M, Gollwitzer H, Harrasser N, Knobloch K, Hausdorf J, Ringeisen M, Gerdesmeyer L. Electromagnetic transduction therapy and shockwave therapy in 86 patients with rotator cuff tendinopathy: A prospective randomized controlled trial. Electromagnetic Biology and Medicine. 2018;37(4):175-183. https://www.tandfonline.com/doi/abs/10.1080/15368378.2018.1499030
- Gerdesmeyer L, Tübel J, Obermeier A, Harrasser N, Glowalla C, von Eisenhart-Rothe R, Burgkart R. Extracorporeal Magnetotransduction Therapy as a New Form of Electromagnetic Wave Therapy: From Gene Upregulation to Accelerated Matrix Mineralization in Bone Healing. Biomedicines. 2024;12(10):2269. https://pubmed.ncbi.nlm.nih.gov/39457582/
Related Topics